
India’s hospital software market is moving from departmental digitisation to platform-level transformation. The India Hospital Management Software Market is projected to grow from USD 12.4 billion in 2025 to USD 25.7 billion by 2031 at a CAGR of 12.8% according to Mobility Foresights. That changes the conversation. Hospital Management Software Development in India is no longer just about replacing paper records or improving billing. It’s about building the operating system for care delivery, compliance, finance, interoperability, and digital growth.
This matters to hospital owners, administrators, CIOs, CTOs, founders of digital health ventures, and healthcare groups expanding across India, the UAE, Europe, the UK, the USA, Singapore, Canada, and Australia. The organisations making the right HMS decisions now are the ones creating cleaner workflows, better data discipline, stronger auditability, and a platform that can support telemedicine, AI, analytics, and cross-border patient services without constant rework.
If you’re evaluating a build, rebuild, or platform migration, this guide gives you a practical view of what works, what usually fails, and what decision criteria matter most. For teams assessing vendors or delivery models, it helps to review Blocsys, its hospital management system services, and its software development cost estimator alongside your internal requirements and procurement process.
Table of Contents
- The Strategic Imperative for Modern Hospital Management Software in 2026
- The Architectural Blueprint of an Enterprise-Grade HMS
- Core Modules Your Hospital Management Software Cannot Ignore
- Navigating the Compliance Maze From ABDM to HIPAA
- HMS Development Roadmap and Cost Analysis for India
- The Future of Hospital Operations AI and Telemedicine Integration
- Why Choose Blocsys for Your Hospital Management Software
- Frequently Asked Questions About HMS Development
The Strategic Imperative for Modern Hospital Management Software in 2026
A 12.8 percent projected CAGR for India’s HMS market through 2031 signals more than software demand. It signals an operating model shift. Hospitals are under pressure to cut revenue leakage, shorten patient wait times, support digital public infrastructure under ABDM, and still meet the expectations of international patients, insurers, and compliance teams.
The strategic question in 2026 is no longer whether a hospital should digitise. It is whether the hospital is building an operating platform that can coordinate clinical, administrative, financial, and compliance workflows without creating new silos.
That distinction matters in practice.
Many hospitals already run multiple systems for registration, billing, diagnostics, pharmacy, claims, and reporting. The result is familiar. Staff re-enter the same patient data, finance teams reconcile mismatched numbers at month-end, clinicians wait on incomplete records, and management gets delayed visibility into occupancy, turnaround time, or unpaid claims. A hospital management system should remove those failure points and create a dependable transaction layer across the institution.
Why procurement has changed
Buying an HMS used to be an administrative decision. Now it is a strategic one tied to margin control, audit readiness, and growth.
Leadership teams are asking different questions:
- Can the system support ABDM-linked interoperability while still meeting stricter expectations from international partners, medical tourism facilitators, or offshore payers?
- Can OPD, IPD, diagnostics, pharmacy, billing, and claims run on the same workflow logic instead of separate databases with manual reconciliation?
- Can management trust the numbers for collections, inventory consumption, denied claims, and doctor-wise revenue without spreadsheet repair work?
- Can the platform handle future requirements such as telemedicine, remote second opinions, clinical analytics, and cross-border data governance?
Hospitals serving foreign patients or planning to expand into medical tourism need to ask one more question early. Can the product design satisfy ABDM participation in India without creating future rework for HIPAA or GDPR controls? That is a system design issue, not a legal footnote.
Practical rule: If the HMS records transactions but does not reduce operational friction between departments, it is digitising paperwork, not improving hospital operations.
What leaders should optimise for
The strongest HMS business case usually rests on four outcomes.
Operational control
Scheduling, admission, diagnostics, ward management, discharge, and billing should follow one governed workflow with clear status changes, ownership, and escalation paths.Financial discipline
In delivery reviews, we regularly find margin loss in three places: claim documentation gaps, charge capture misses, and consumables that move faster than they are recorded. A good HMS reduces those gaps through workflow controls, not only reports after the fact.Compliance by design
Audit logs, consent records, role-based access, retention rules, and interoperability standards need to be part of the product architecture from the start. Teams planning for both Indian and international operations should map data movement carefully. A hospital data pipeline architecture built for healthcare interoperability helps avoid expensive redesign later.Strategic flexibility
Hospital software should support expansion into new sites, partner ecosystems, analytics programs, and research use cases without forcing a full rebuild. Teams working on longitudinal data or research-grade normalization can review OMOPHub’s FHIR to OMOP resources when planning secondary use of clinical data.
For administrators, the priority is operational reliability. For CTOs, the priority is change tolerance over a five to seven year horizon. The right HMS does both. It supports the discipline required by ABDM in India and the control model expected under HIPAA or GDPR for global-facing care delivery.
The Architectural Blueprint of an Enterprise-Grade HMS
A hospital system becomes fragile when architecture follows departmental silos. It becomes durable when architecture follows data, permissions, and clinical workflow. That distinction matters more than whether a vendor’s demo looks polished.
Choose architecture based on operational complexity
A small hospital may still run effectively on a tightly managed modular core. A large multi-specialty hospital usually needs clearer service separation, stronger integration discipline, and better fault isolation.
The most useful architectural choices typically sit along these lines:
- Cloud-based deployment works well when leadership wants faster rollout, easier scaling, and lower infrastructure management overhead.
- On-premise deployment can still make sense where internal policy, legacy integration, or data residency constraints drive that decision.
- Microservices architecture is better suited to environments where pharmacy, billing, lab, and patient services need to evolve independently.
- Monolithic architecture can be acceptable for narrow scope systems, but it often becomes expensive to modify once the hospital adds more departments and integrations.
A good HMS should expose a disciplined API layer. That’s what allows appointment systems, billing engines, LIS, pharmacy, EMR workflows, and external services to exchange information without brittle custom scripting.
Design around data flow, not just modules
Most implementation pain comes from bad handoffs. Registration creates one patient record. Lab uses another format. Billing uses a third. Insurance teams patch over the gaps. That’s how hospitals end up with operational chaos inside a system that was supposed to create order.
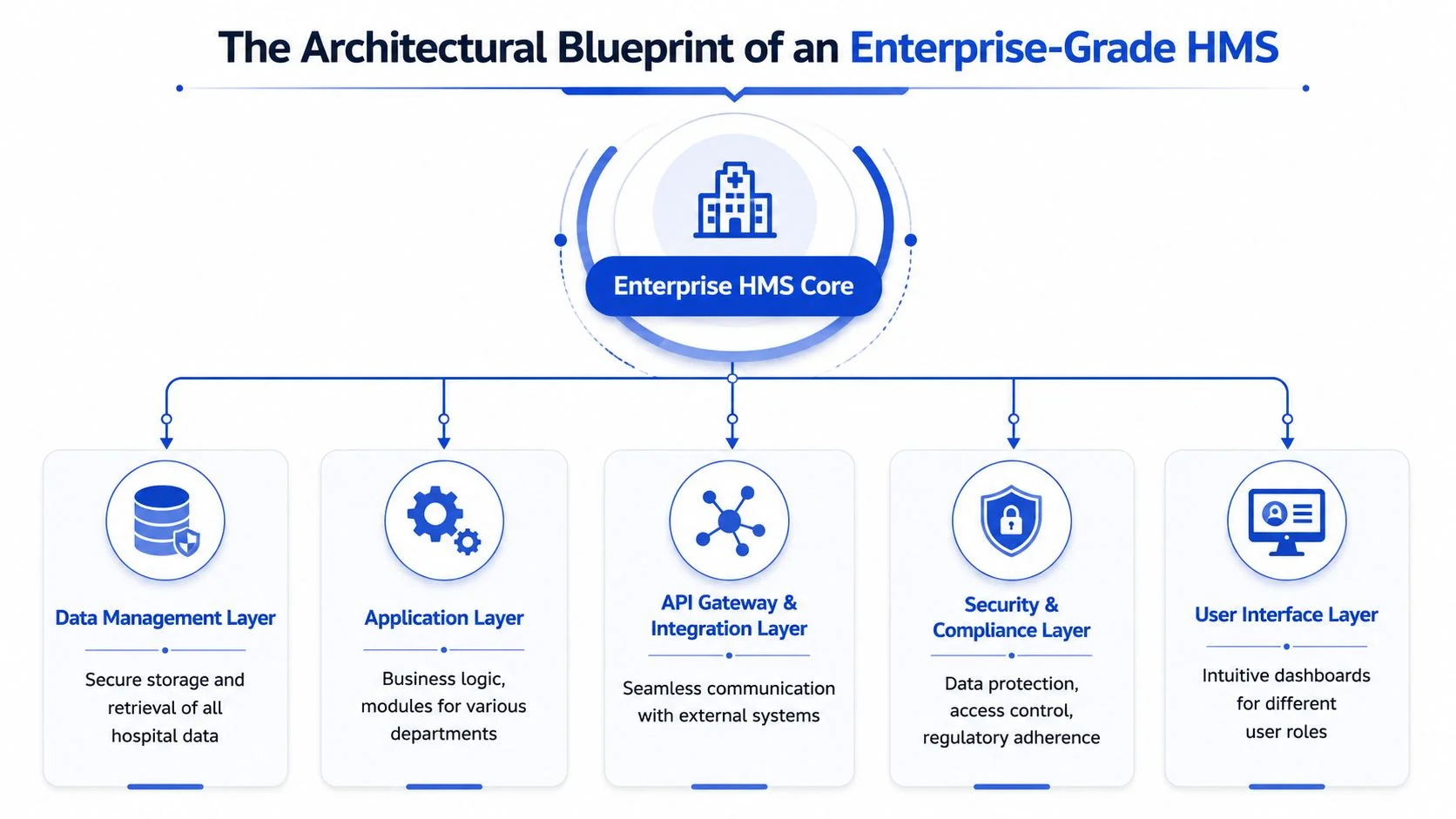
The better model is a central data strategy with role-based application services layered on top. That architecture usually includes:
| Layer | What it should do |
|---|---|
| User interface layer | Serve reception, clinicians, nurses, pharmacists, finance teams, administrators, and patients with role-specific views |
| Application layer | Handle business logic for OPD, IPD, pharmacy, billing, lab, radiology, discharge, and claims |
| Data management layer | Maintain secure and consistent storage of patient, operational, and financial data |
| API and integration layer | Connect internal modules and external systems using controlled interfaces |
| Security and compliance layer | Enforce authentication, authorisation, encryption, audit logging, and policy controls |
For teams mapping health data into research or analytics environments, OMOPHub’s FHIR to OMOP resources are useful because they highlight the practical translation issues that appear once interoperability moves from theory to implementation. Internally, healthcare teams also benefit from thinking through data pipeline architecture early, because reporting, AI models, and external data exchange all depend on clean upstream design.
The architecture should make it hard to create bad data, not just easy to enter more data.
Core Modules Your Hospital Management Software Cannot Ignore
Hospitals often ask for an all-in-one platform, but implementation success usually depends on getting a small set of modules absolutely right first. If registration is weak, every downstream process suffers. If pharmacy and billing are disconnected, stock discipline and revenue integrity both break.
The modules that carry the hospital day
Patient registration and appointment scheduling form the front door. The system should handle identity capture, repeat visits, queueing, doctor availability, and specialty-level scheduling rules. In practice, a key benefit is continuity. Staff shouldn’t have to recreate patient records because one department captured data differently from another.
Doctor and staff management does more than roster planning. It affects consultation allocation, procedure scheduling, leave visibility, privileges, and accountability. When this module is weak, overbooking and poor utilisation become routine.
Pharmacy and inventory management should link prescribing, dispensing, stock movement, batch tracking, and purchase workflows. Hospitals that separate prescribing from dispensing records often create avoidable medication and reconciliation problems.
Laboratory management needs structured order flow, sample tracking, result entry, verification, and status updates visible to clinicians and billing teams. The operational value comes from reducing blind spots between test ordering and report availability.
Billing and insurance administration must work as a transactional spine, not a separate finance tool. Charges should flow from consultations, procedures, pharmacy, bed allocation, diagnostics, and packages with clear insurance logic and claim support.
A document trail also matters. For consent forms, discharge papers, legal records, and audit-sensitive artefacts, technologies such as blockchain document verification for healthcare, legal, and government records can be relevant where hospitals need tamper-evident verification rather than basic file storage.
Hospitals usually don’t need more modules first. They need fewer workflow breaks.
EMR vs EHR What’s the difference
The terms get used interchangeably, but they aren’t the same. That confusion causes procurement errors.
| Aspect | Electronic Medical Record (EMR) | Electronic Health Record (EHR) |
|---|---|---|
| Scope | Typically focused on records within one provider or facility | Designed for broader sharing across providers and care settings |
| Primary use | Clinical documentation and treatment history inside the organisation | Continuity of care across organisations and systems |
| Data exchange | Often more limited unless specifically integrated | Built with interoperability expectations in mind |
| Typical users | Doctors, nurses, and internal clinical teams | Broader care ecosystem, including external providers where permitted |
| Strategic role | Improves internal clinical workflow | Supports connected care and longitudinal patient history |
The practical answer is simple. A modern HMS should support both internal clinical workflow and structured data exchange. If your platform treats EMR and EHR as separate future projects, it usually means the data model wasn’t designed properly at the start.
Navigating the Compliance Maze From ABDM to HIPAA
Cross-border care changes the compliance burden fast. An HMS built for Indian hospital operations alone will usually fall short once the same institution starts serving international patients, sharing records across jurisdictions, or supporting telemedicine beyond India.
For hospitals targeting medical tourism or global specialty care, compliance is not a legal checklist added after deployment. It is a system design decision that affects patient identity, consent capture, API structure, data residency, audit trails, breach response, and vendor selection from day one.
Dual compliance changes the system design
ABDM pushes hospitals toward standardised identifiers, consent-aware exchange, and FHIR-aligned interoperability. That directly affects how the HMS stores patient demographics, structures clinical records, exposes APIs, and records consent events across OPD, IPD, diagnostics, pharmacy, and claims workflows. A system that treats ABDM as a later integration task usually ends up with expensive rework.
HIPAA and GDPR raise a different set of questions. Who can access what data. Where is that data stored. How quickly can the hospital produce an access log, revoke permissions, respond to a breach, or fulfil a patient data request. These are architecture questions, not policy documents.
This is the trade-off hospital leadership needs to understand. A locally optimised HMS may help teams move faster in the short term. A globally viable HMS needs stricter data classification, clearer access controls, better logging, and tighter vendor governance.
India-based providers working through overlapping privacy obligations should also examine GDPR, DPDP Act, and blockchain document verification compliance challenges because international patient flows rarely stay inside one legal framework.
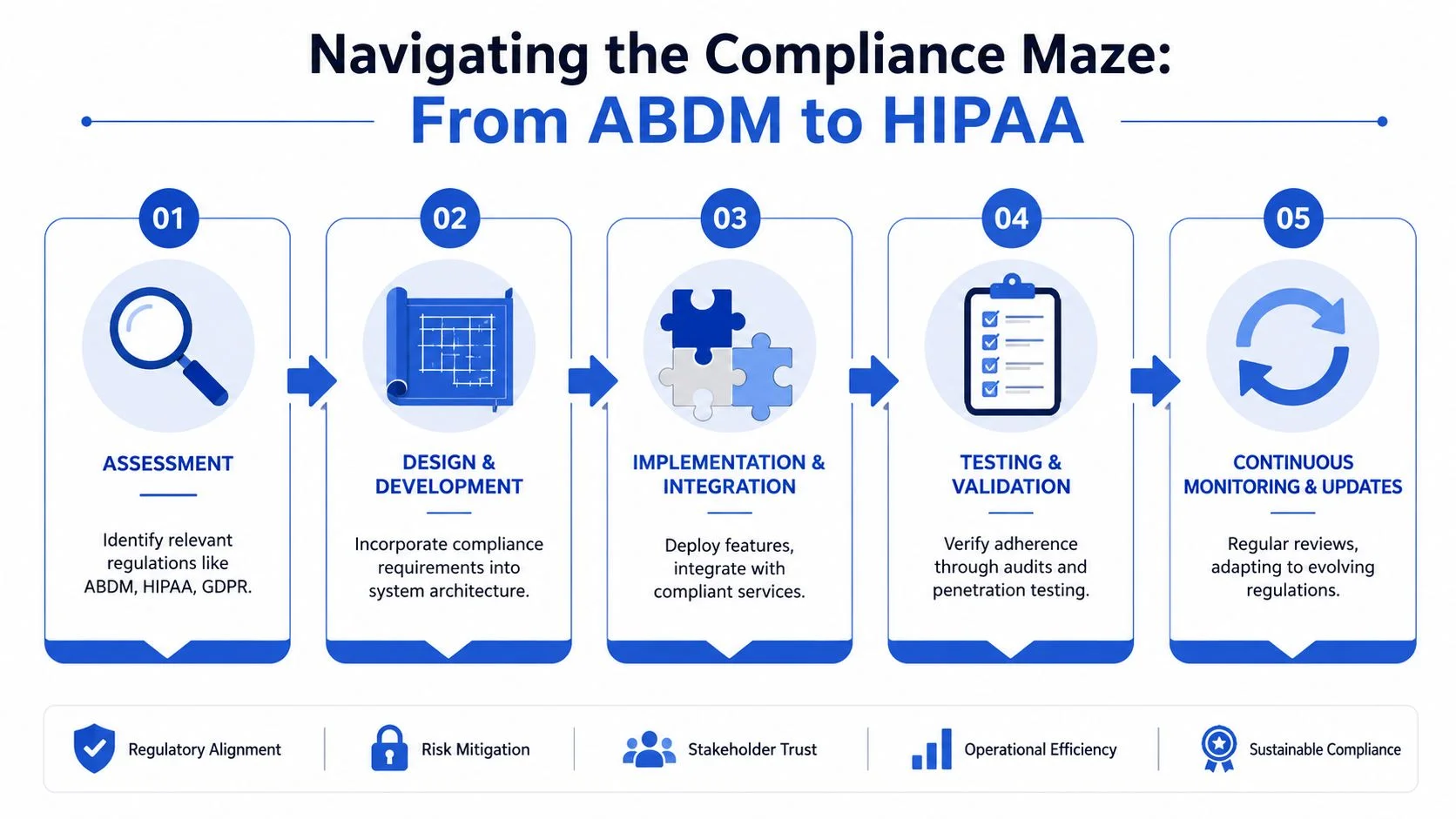
What a workable compliance model looks like
The practical model is to split the platform into shared controls and jurisdiction-specific rules. That keeps the core platform maintainable while allowing legal and operational differences by geography.
- Shared controls should cover identity and access management, encryption at rest and in transit, session controls, API security, immutable audit logs, backup policy, and incident monitoring.
- ABDM-specific rules should cover patient identity mapping, consent artefacts, FHIR resource compatibility, health record exchange, and Indian administrative reporting requirements.
- HIPAA and GDPR-specific rules should cover minimum necessary access, disclosure tracking, retention schedules, breach workflows, cross-border transfer rules, and data subject rights handling.
In practice, this usually means role-based access is not enough. Enterprise hospitals need attribute-based controls for department, location, care context, insurer relationship, and patient consent status. They also need audit logs that can stand up in an investigation, not just logs that satisfy developers during testing.
A useful benchmark comes from healthcare engineering teams that emphasise encryption, multi-factor authentication, secure transfer methods, static code analysis, penetration testing, and alignment with standards such as ISO 27001 and HIPAA, as described by Tata Elxsi’s healthcare software engineering overview. Those controls matter because hospitals do not get judged on policy intent. They get judged on evidence.
Compliance architecture should be visible in permissions, logs, and data flows. If the system cannot show who accessed a record, under what rule, and where that data moved, the hospital will struggle in an audit.
HMS Development Roadmap and Cost Analysis for India
Budget conversations become more productive once hospitals stop asking “what does software cost?” and start asking “what scope are we funding?” HMS pricing depends on bed size, module breadth, integration needs, security expectations, and implementation discipline.
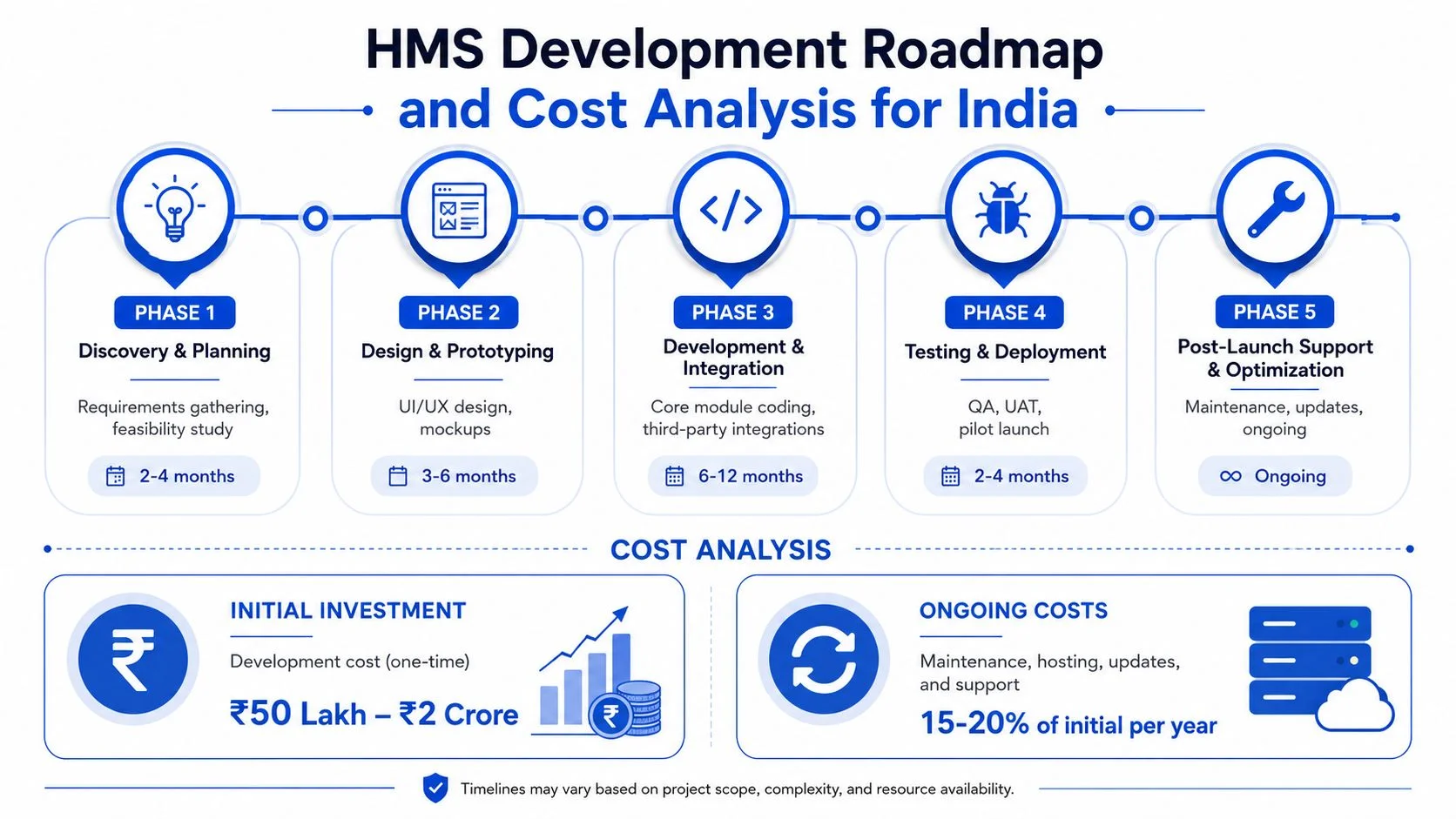
What Indian hospitals should budget for
In the Indian market, custom HMS development in 2026 ranges from ₹6–15 lakh for small hospitals with 10–30 beds over 3–6 months, while enterprise hospitals with 150+ beds typically require ₹35–70 lakh+ over 12–18 months, with recurring hosting and maintenance costs on top, according to OneCity’s HMS cost guide.
The same benchmark also distinguishes scope by complexity:
| Hospital type | Typical build scope |
|---|---|
| Clinic or small hospital | Core registration, appointments, billing, and basic operational modules |
| Mid-size hospital | Adds IPD, lab, radiology, and insurance or TPA workflows |
| Enterprise hospital | Expands into ICU, OT, PACS or DICOM, executive BI, and AI-enabled decision support |
That’s why comparing vendor quotes without a module map is a mistake. One proposal may include only transactional workflows. Another may include interoperability, analytics, and enterprise security layers that change long-term value significantly.
A practical delivery roadmap
Most successful projects move through a disciplined sequence rather than trying to launch every module together.
Discovery and workflow mapping
Document departments, exceptions, approval paths, and reporting needs before screens are designed.Platform design
Finalise architecture, data model, user roles, and integration requirements.Core module build
Start with the operational spine, usually registration, appointments, billing, pharmacy, and selected clinical workflows.Integrations and hardening
Connect lab, radiology, accounting, insurance, and external data exchange points. Then test permissions, auditability, and failure scenarios.Pilot, rollout, and optimisation
Launch in controlled phases, train users by role, and refine based on actual floor-level usage.
Before procurement starts, finance and technology teams should use a structured estimator such as estimate development costs before you hire developers to align budget expectations with module scope and rollout ambition.
The Future of Hospital Operations AI and Telemedicine Integration
The next generation of HMS won’t be judged only by whether it records events accurately. It will be judged by whether it helps hospitals act earlier, schedule better, and operate with less friction.
AI is most useful when it sits inside workflow
AI in healthcare operations works best when it supports a specific decision inside an existing process. Useful examples include triage support, anomaly detection in operational data, bed and resource forecasting, documentation assistance, and clinical decision support embedded into care pathways.
That means the HMS has to provide clean, structured, permissioned data. Without that foundation, AI becomes a dashboard exercise rather than an operational capability. Hospitals exploring this path usually need a development partner that understands both healthcare workflows and AI and ML development services at production level.
Telemedicine only works when core operations are connected
Telemedicine often gets treated as a separate front-end product. That’s a common mistake. Remote consultations still depend on patient identity, scheduling, clinician availability, prescriptions, diagnostic orders, follow-ups, payment capture, and medico-legal documentation.
For revenue-linked workflows, it also helps to understand how automation is changing collections, claims discipline, and billing operations more broadly. Teams evaluating those operational dependencies can review 2026 revenue cycle management insights from Happy Billing as a useful reference point for where integrated automation is heading.
The hospital that wins with telemedicine usually isn’t the one with the nicest video interface. It’s the one that connects virtual care to the same operational backbone as in-person care.
Over the next 12 to 24 months, hospitals that invested in composable, secure HMS platforms will be in a stronger position to roll out AI-supported workflows and cross-channel patient services without rebuilding their core systems.
Why Choose Blocsys for Your Hospital Management Software
Hospital groups rarely fail on software selection because a vendor cannot show enough screens. They fail because the platform does not hold up under real operating pressure across admissions, billing, pharmacy, diagnostics, insurer workflows, discharge coordination, and audit requirements.
Blocsys is a Pune, Maharashtra based firm incorporated in 2021. Its HMS offering covers patient registration, discharge, pharmacy, lab operations, insurance claims, and an accounting ledger aligned with Tally, as noted earlier in the article. For Indian hospitals, that matters because financial control often breaks at the handoff points between clinical activity and billing, not inside a single department.
The stronger reason to consider Blocsys is architectural fit. A hospital serving domestic patients, corporate accounts, insurers, and international medical travelers needs one platform that can handle Indian workflow realities while still supporting stricter expectations around security, auditability, consent handling, and cross-system interoperability. That balance is difficult. Many vendors understand local operations but not international compliance exposure. Others know enterprise software but miss how Indian hospitals run in practice.
Blocsys is more relevant for buyers who need a practical middle path. The company works across healthcare software, AI, blockchain, and enterprise systems, which is useful when the HMS is expected to do more than manage appointments and billing. Hospitals planning ABDM-aligned interoperability and also preparing for HIPAA or GDPR-sensitive use cases should evaluate whether the vendor can separate data access by role, maintain reliable audit logs, support integration layers cleanly, and extend the product without rewriting the core platform.
Selection should come down to execution questions. Can the vendor map current workflows before customisation begins? Can finance, clinical, and administrative data stay consistent across modules? Can the system support future API integrations, reporting demands, and controlled deployment in multi-location environments? Blocsys is one option worth assessing against those criteria, especially for healthcare organisations that want an HMS with room for compliance-heavy growth rather than a short-term departmental tool.
Frequently Asked Questions About HMS Development
What is Hospital Management Software
Hospital Management Software is the digital platform that manages hospital workflows such as registration, appointments, admissions, billing, pharmacy, lab, discharge, reporting, and administrative control. A strong HMS connects departments so data moves with the patient journey instead of being re-entered at every step.
How much does Hospital Management Software Development cost in India
Costs depend on hospital size and module scope. In India, custom HMS development in 2026 ranges from small-hospital builds to enterprise platforms with broader clinical and operational coverage, as detailed earlier from the cited Indian market benchmark.
Can HMS integrate with EMR, EHR, and telemedicine
Yes, but only if the data model and API layer are designed properly. Integration shouldn’t be treated as an afterthought. The system has to support clinical documentation, interoperable record exchange, scheduling, consultation workflows, and secure communication across channels.
How secure should a modern HMS be
It should include encryption, role-based access, multi-factor authentication, audit logs, secure APIs, regular testing, and controlled data transfer practices. In hospitals serving international patients, security design also needs to reflect external compliance obligations.
If you’re planning Hospital Management Software Development in India for a clinic, hospital group, diagnostic network, or global healthcare venture, connect with Blocsys Technologies for practical guidance on architecture, compliance, cost planning, EMR or EHR integration, telemedicine, AI healthcare applications, and custom healthcare software execution.